Techniques for delivering smart adaptive radiotherapy
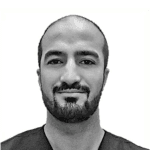
IMRT has been the gold standard technique for delivering radical radiation to most tumour sites for at least a decade. It is three-dimensional radiotherapy; plans sculpt dose towards the disease and away from organs at risk (OAR) in all three axes. These shapes are defined by the patient’s geometry at a single timepoint – the planning CT scan. However, differences in day-to-day set-up, weight loss, external shape change and gain or loss in the volume of both tumours and OARs means that the radiation dose that is eventually delivered to these structures may differ from that which was anticipated at planning. An example is shown in figure 1, in which the dose plan for a head and neck patient is super-imposed on first and final fraction images. Image guidance (IG) can mitigate some of these effects, but even with optimal IG protocols delivered dose may not be the same as planned, and research is ongoing to understand how clinically significant these differences might be.
The content on this page is provided by the individuals concerned and does not represent the views or opinions of RAD Magazine.