AECC University College provides insights into spine instability

New research from AECC University College’s Centre for Biomechanics Research suggests that the current standard of using end of range x-rays for selecting patients with instability for fusion treatment cannot be relied upon.
Patients with chronic low back pain are sometimes considered for back fusion surgery if sliding between their vertebrae, measured from x-rays taken at the beginning and end of bending, exceeds 3mm. However, many surgeons and other clinicians have expressed scepticism and concern about the amount of sliding that can actually be detected using this method. This is because the motion between vertebrae during bending is never exactly the same if repeated, nor is its maximum always at the end of trunk bending. Therefore, because there will always be some error, stabilisation surgery on the spine, which is not reversible, cannot easily be justified without knowing its magnitude.
The research, published online in Scientific Reports, assessed the error associated with measuring instability of the spine using end of range x-rays. This was compared to a more advanced and standardised dynamic method that uses the whole range of motion to measure the greatest amount of sliding, wherever it occurs during bending. Fifty-five volunteers with no back pain had measurements taken using both methods and repeated six weeks later, to find out how repeatable they were.
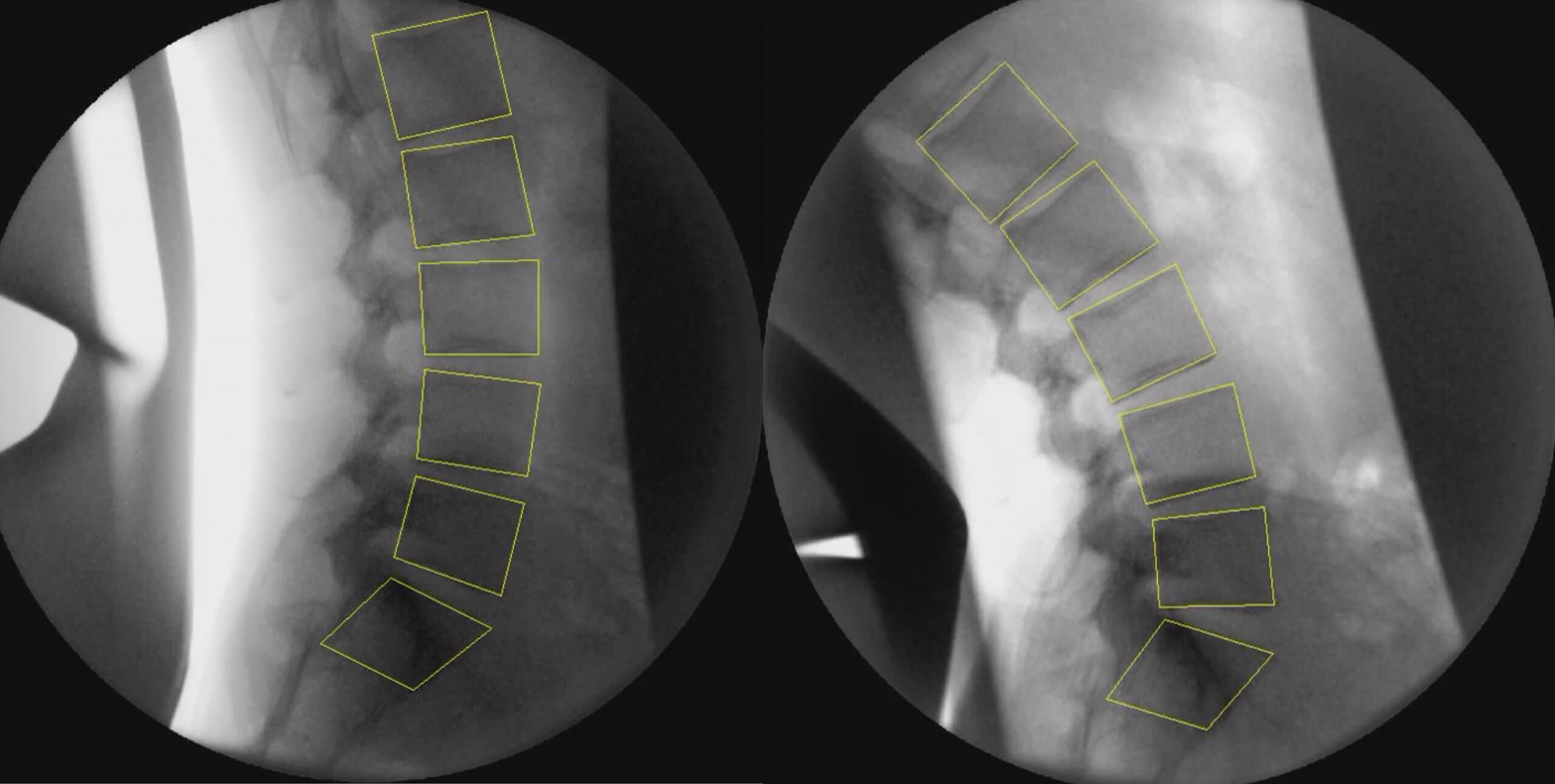
The results showed that the smallest change that can be detected using end of bending x-rays is up to 4mm, compared to 2mm using the dynamic, standardised motion method. The new method uses fluoroscopy and computer analysis of over 300 consecutive images.
This study demonstrated that the previously accepted criterion of 2.8mm of sliding measured using end of range x-rays for selecting patients with instability for fusion treatment cannot be relied upon and a quantitative fluoroscopic examination would be necessary to meet this standard.
Published on page 9 of the February 2020 issue of RAD Magazine.